
A nosology is a system of disease classification, and the National Institute of Mental Health (NIMH) is promoting a new one, the Research Domain Criteria (RDoC). Yesterday, Childhood Obesity News outlined the basic characteristics of the systems already in place, the Diagnostic and Statistical Manual of Mental Disorders (DSM) and the International Classification of Diseases and Related Health Problems (ICD). Karen Franklin, Ph.D., forensic psychologist and adjunct professor at Alliant University in Northern California, says:
Mental health professionals know not to take the DSM (or the ICD, for that matter) too seriously. It’s just convenient fiction, or at best “useful constructs,” mainly used to attain insurance reimbursement….
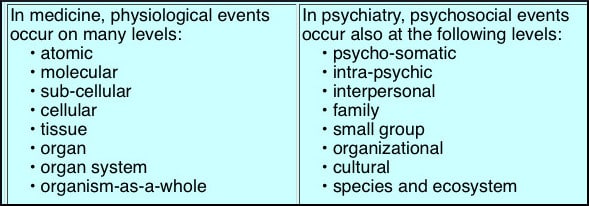
We also touched on case formulation, the preferred diagnostic approach of some healers. The illustration on this page is a chart from Dr. Adam Blatner’s “The Art of Case Formulation,” which serves to remind us of just how many different things might play a part in any given illness. Unfortunately, being such an art, case formulation is not eminently suited to the modern need for speedy and concise information delivery. NIMH realizes that diagnostic science is not keeping up. Because mental function depends on multi-layered systems, new ways are needed to classify mental disorders based on both observable behavior and neurobiological test results. Dr. Franklin reminds us:
Remember when they first announced work on the new DSM? It was going to be a revolutionary “paradigm shift,” aligning diagnoses with modern science. Disorders were going to be dimensional rather than categorical…
But it didn’t happen. To give an example of the difficulties that impact childhood obesity, here is a problem that did not disappear with the new DSM revision:
While the DSM-IV uses a categorical classification system of mutually-exclusive diagnoses, patients with eating disorders often develop symptoms consistent with more than one diagnosis over the course of their illness, demonstrating shifts between diagnoses known as diagnostic crossover.
According to those who want change, DSM and ICD are perceived as too rigid. In the legal system, which clings to the DSM with fervor, Dr. Franklin points out that “the consequences of error can be grave.” But the real burr under the saddle is that, in the United States, the DSM has a stranglehold on the research grant application process. Dr. Bruce Cuthbert says, “The whole machinery of science is governed by the DSM.” The call for change, then, is a demand for more useful research standards and criteria.
To educate mental health professionals about RDoC, the federal mental health agency set up a webinar to explain its preferred new way of categorizing mental disorders. The initiative is led by Dr. Cuthbert, who introduces, “the guiding principles… the role of the new RDoC unit, and frequent questions researchers have….” Here is the best part—the 47-minute presentation is viewable by the public!
The new RDoC is touted as a flexible tool capable of achieving a happy medium. At first blush, it does sound as if RDoC is more conscious of all the possibilities listed in Dr. Blatner’s chart of physiological and psychosocial factors. But there is another point of view, capably represented by Dr. Franklin, who opines that:
Switching to its biology-worshipping Research Domain Criteria is like jumping from the frying pan to the fire.
Your responses and feedback are welcome!
Source: “DSM-5: Forensic applications (Part II of II),” Blogspot.com, 05/30/13
Source: “The Art of Case Formulation.” Blatner.com, 09/15/06
Source: “NIMH Webinar Explains New Way of Categorizing Mental Disorders,” madinamerica.com, 12/06/14
Source: “DSM-5: Much ado about nothing? (Part I of II),” Blogspot.com, 05/29/13
Source: “Cognitive Behavioral Therapy for Weight Management and Eating Disorders in Children and Adolescents,” NIH.gov, 04/01/12
Image by Adam Blatner, MD
 FAQs and Media Requests:
FAQs and Media Requests: 











